Heartburn, Indigestion, Reflux:
Is There A Cure?
 I avoid spicy food when I have a sore throat because it intensifies my pain. But why? Raw, swollen, inflamed tissues are more sensitive to irritation. And there you have it. For any two people experiencing the same amount of food regurgitation from the stomach to the esophagus, the one with sickly inflamed tissues will report the greatest symptoms and will go on to the greater complications of gastroesophageal reflux disease (abbreviated GERD, Gastro refers to your stomach, the esophagus is the tube connecting your mouth to your stomach, and reflux is the return of food and drink back up the esophagus from the stomach usually with acid in it which burns the esophagus and causes pain). In the rest of this discussion I will refer to heartburn, indigestion, and reflux collectively as GERD.
I avoid spicy food when I have a sore throat because it intensifies my pain. But why? Raw, swollen, inflamed tissues are more sensitive to irritation. And there you have it. For any two people experiencing the same amount of food regurgitation from the stomach to the esophagus, the one with sickly inflamed tissues will report the greatest symptoms and will go on to the greater complications of gastroesophageal reflux disease (abbreviated GERD, Gastro refers to your stomach, the esophagus is the tube connecting your mouth to your stomach, and reflux is the return of food and drink back up the esophagus from the stomach usually with acid in it which burns the esophagus and causes pain). In the rest of this discussion I will refer to heartburn, indigestion, and reflux collectively as GERD.
What are the signs and symptoms of GERD?
The top 10 common symptoms for GERD are as follows:
- Reflux (the return of food and drink back up the esophagus).
- Acid regurgitation (excessive acid or sour taste in the food coming back up the exophagus).
- Postprandial fullness (bloating in the stomach area after a very large meal).
- Heartburn (pain in the chest).
- Swallow obstruction or pain (feeling that you can’t get the food to go down).
- Epigastria burning sensation (Burning pain in the stomach area).
- Paraesthesia pharynges (sore or full filling throat).
- Post sternal pain (pain behind the breast bone).
- Chronic laryngopharyngitis (hoarseness, sore voice box and sore throat).
- Chronic cough (a never ending caugh).[1]
How common is GERD?
Prevalence of Gastro Oesophageal Reflux Disease is as follows:
- 18.1%–27.8% in North America.
- 8.8%–25.9% in Europe.
- 2.5%–7.8% in East Asia.
- 8.7%–33.1% in the Middle East.
- 11.6% in Australia.
- 23.0% in South America.[2]
So, if you are experiencing GERD, you are not the only one, others have been through this, it has been extensively studied, and knowing the causes goes a long way toward directing one’s efforts at relieving and healing the problem.
What Causes GERD?
Let’s look at the different mechanisms involved in digestive pain that is associated with disorders of the esophagus and stomach. We’ll look at the system as a whole and also at individual parts.
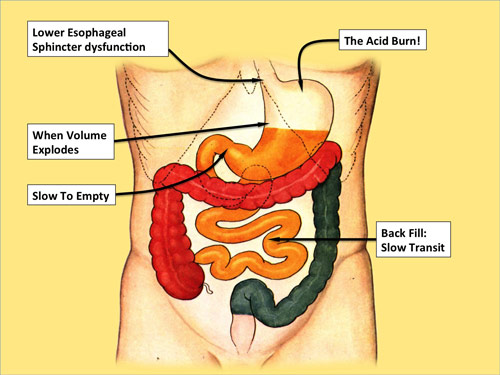
The Lower Esophageal Sphincter
The first thing that can happen involves a poorly closing valve at the lower end of the esophagus, immediately on top of the stomach. This is referred to as the lower esophageal sphincter. Anything that compromises its ability to close tightly can lead to acid laden stomach contents regurgitating up into the esophagus causing pain, acid tissue burn, open sores, ulceration, or even pre-cancerous conditions. There is a long list of things that are proven to compromise lower esophageal sphincter function.
These include:
- High fat foods.[3]
- Whole Milk.[4],[5]
- Soups.[6]
- Chocolate.[7]
- Coffee.[8]
- Tea.[9]
- Nicotine.[10]
- Alcoholic beverages.[11]
- Peppermint.[12]
- Colonic Fermentation (when you eat foods that tend to rot in the colon).[13]
- Soda Drinks.[14]
The Acid Burn
Then next consideration in painful reflux disease (GERD) is the lifestyle habits that increase the acidity of the stomach or that acid’s access to the esophagus.
Anything that increases the acidity of the stomach contents makes them that much more likely to cause pain and damage when they regurgitate up into the esophagus.
The list of things that increase the acid burn include many things. Any Autoimmune inflammatory disease or process, as we discussed in the beginning of our paper, weakens the tissues, making them more vulnerable to acid damage.[15],[16],[17] This includes allergies, such as having a milk allergy.[18]
Some foods, by their very nature, increase inflammation and stomach acidity. Research has shown that certain spices do this and include: red and black pepper,[19] fennel, cardamom, cumin, coriander,[20] and Curry.[21]
Some foods are naturally high in acid content and pose a problem for many people, citrus[22] and soft drinks[23] for example.
If you are having GERD symptoms and are on other medications, it would be possible that some of these are the cause of your heartburn.[24],[25]
Salt[26] and sugar as well as refined carbohydrates[27],[28],[29] can increase the acid burn.
If you have a choice between canned and fresh foods, fresh foods are the better choice for avoiding GERD.[30]
I don’t know if you count calories, but be aware that foods high in calories and low in fiber or bulk are well know to increase acid reflux. [31] We call these foods high caloric density foods.
Not only do high fat foods relax the lower esophageal sphincter, they also increase the stomach acid, [32] mostly because they are hard to digest.
Fast foods[33] are poor nutrition for the most part and increase the acid burn.
If you are going to eat something, you might as well chew it well, this will help in your fight against an acid stomach.[34],[35]
Regular meals are helpful, on the other hand snacking is not in your best interest. [36],[37]
Certain stimulants are known to increase the acid burn. These include tea, coffee, caffeine,[38] and alcohol.[39]
The more concentrated the acid in your stomach the worse the burn, on the other hand diluting out the acid with good hydration of the tissues is beneficial, so avoid dehydration.[40] Drink you water at least one half hour before meals or two hours after meals to avoid GERD.
You may be thinking you are doing your self a favour by taking calcium based “anti-acids” but in reality they only produce what we call the acid rebound, resulting in more acid in the long run and more reflux.[41],[42]
You are what you eat; eating good food favours strong, healthy, resilient tissues resistant to acid damage. On the other hand malnutrition[43] is dangerous, it weakens the lining of the stomach and esophagus and compromises their mucosal integrity.[44]
Perfect health depends on perfect circulation, this means good blood supply. Poor blood supply[45],[46] compromises the lining of the stomach and esophagus, making them unable to properly repair tissue damage.
When you overeat, making your stomach into a tightly filled balloon, it stretches the esophagus lining into the stomach where it does not belong, exposing it to the acid of the stomach. This creates the same pain and tissue compromise as regurgitation.[47]
Now if you worry[48] too much, and your stress levels rise, [49] this also increases the vulnerability of the digestive tissues to damage and the stomach’s production of acid.
Over Filling The Stomach
If the stomach could be quickly emptied after meals, the chance that it would reflux would be greatly reduced. On the other hand, keeping the stomach exceedingly full only increases the likelihood of GERD. If you do not want your stomach to remain full for a long time, eat less. Overeating[50] only produces distension, slow digestion and reflux. Think of it like a front loader washing machine. If you pack the machine totally full, it cannot agitate the clothes and the laundry cannot get clean. Filling the stomach only partially full leaves it room to mix the foods with digestive juices and complete its digestion in a reasonable amount of time. “And put a knife to thy throat, if thou be a man given to appetite.”[51]
The digestion is severely slowed and compromised by eating between meals or snacking.[52] Meals should be at lease 5 hours apart. Eating too frequently (<5hr between meals)[53] causes stacking of the meals, stomach overfilling and overflow, i.e. reflux. If your toilet overflows you figure you must have put too much in it. The same is true of reflux. If things keep on coming up (refluxing), stop putting so much down, and give the food time to move on in between meals.
Foods eaten to quickly overcrowd the stomach and can result in reflux.[54]
Studies now show that foods eaten without proper chewing in the mouth take longer to digest in the stomach.[55] Your stomach does not have teeth. It can only add acid and agitate the food.
Some people take on more than just food at a meal, they add liquid as well. This liquid is more likely to regurgitate up into the esophagus. It also makes the stomach take longer to move the food on to the small intestines because before it can get on with the process of digestion it must absorb the liquid. This is true of drinks with meals and of liquid foods, like soup, smoothies, porridges and juices.[56]
Emptying the Stomach
The stomach can be quickly cleared of food only as the food is of good quality and well chewed. Certain foods and lifestyle practices delay the emptying of the stomach these include:
- High fat[57],[58] or fried foods.[59]
- High caloric density foods.[60]
- Chilled/refrigerated cold food or very hot food.[61]
- Nicotine or tobacco.[62]
- Alcohol.[63]
- Liquid taken with your meals.[64]
- Supplement tablets can delay stomach emptying.[65]
- Snacking between meals or meals too close together.[66]
- Laying down after a meal.[67]
- Eating in the evening leaving less than 3 hours before going to bed.[68]
- Autoimmune inflammatory gastritis.[69]
- Intense exercise after eating.[70]
- Mental stress.[71]
Slow Intestinal Transit
If there is no room beyond the stomach in the digestive system, food cannot be transferred out of the stomach and reflux is more likely to result. Some foods and lifestyle habits produce a condition we refer to as slow transit, it could also be referred to it as back fill.[72] It could be compared to a traffic jam or even rush hour traffic.
Things that slow intestinal transit are many. Refined foods, like white flour[73] cause this problem because they are low in fiber.[74]
Because low fiber food is in the colon so much longer, bacteria tend to multiply,[75] This results in bacterial overgrowth. When bacteria over grow they produce many toxins[76] and inflammation. [77]
Slow transit foods are usually high in fat and low in fiber, and include meat, fast foods, pastries, especially donuts, fried foods and greasy foods[78].
Foods eaten late at night tend to pass more sluggishly through the digestive system thus they have the same effect of fostering bacterial overgrowth[79].
Fiber plays a significant role in the time food stays in your system[80]. Whole grains[81], dried fruit[82] and fresh vegetables are good sources of dietary fiber. What is people’s favourite high fiber dried fruit eaten to help improve stool consistency and shortened transit time? Prunes, right? Have you heard it said, “With friends like prunes, who needs enemas”?
High fat foods have been shown to slow intestinal transit.[83]
Juice, probably because of the removal of fiber, slows transit.[84]
Mental health can also effect transit times, depression tends to slow transit and make digestion sluggish[85].
The back pressure exerted by tight clothing, such as a belt,[86] can significantly slow the rate at which food makes it out of your intestines.
Exercise tends to quicken bowel movement whereas a sedentary lifestyle has been shown to slow transit time. [87],[88]
Dietary Gluten[89],[90] and dairy products[91] cause a sluggish colon and slow transit times.
Of all the diets studied, that cause multiple health issues, the western diet, of meat, high fat foods, cheese and refined grains tops the list. And it contributes to slowed transit of food through the entire digestive system.[92],[93]
Nothing slows transit time quite like constipation[94] for which increased water and fiber intake are often the antidote.
Gas or flatulence block the way for food to pass on down the digestive tract and slow transit times.[95]
If your posture is poor and you are always doubled over, the effect is like that of the tight belt, it creates intestinal backpressure, which slows transit time.[96]
So keep the food moving for reduction in risk of reflux at the other end.
Epidemiological Associations
Some foods and lifestyle factors have been found to increase the likelihood of reflux, dyspepsia or heart burn, but the actual mechanism may not yet be well understood. These include:
- Milk, lettuce, brewer’s yeast, pork, coffee, rice, asparagus, and tuna, followed by eggs, tomato, grain, shrimps.[97]
- Animal protein/meat.[98],[99]
- Vinegar.[100],[101]
- Late supper.[102]
- Low dietary magnesium intake.[103]
- Low Dietary Vitamin C.[104]
- Obesity.[105]
- Medical drugs.[106]
- Psychological stress.[107]
- Improper chest breathing.[108]
- Cheese causes gastritis.[109]
Barrett’s Esophagus
When the esophagus receives repeated acid burns and becomes raw and inflamed cancer becomes a big risk. This condition of the esophagus has been given the name Barrett’s esophagus. Some foods and lifestyle factors have been identified as high risk or causal in Barrett’s esophagus and cancer. These include:
- Sugar.[110],[111]
- Smoking, abdominal obesity, and a Western diet.[112]
- Inflammatory diet.[113]
- Late evening meal.[114]
- Low fiber diet.[115]
- Pizza.[116]
- Wearing a belt.[117]
- Meat and saturated fat.[118]
- Dark green vegetable deficiency.[119]
- Low dietary vitamin A.[120]
- Low Dietary Vitamin C.[121]
- Diet low in fresh fruits and vegetables.[122]
- High animal-fat intake.[123]
- Smoking.[124]
- Selenium deficiency.[125]
- Diet rich in cereal but poor in fresh fruit and vegetables.[126]
- Processed meat consumption.[127]
How is GERD Generally Treated?
GERD is usually treated by a medical doctor with a medication, which in most cases is continued indefinitely. Ninety-five precent of patients are prescribed a drug of which 83% are proton pump inhibitors or PPIs, medications designed to reduce the stomachs ability to produce acid.[128] Between 1995 and 2006 there was a 1318% (over 12 times) increase in proton pump inhibitors prescribed in Australia for people with GERD.[129] Proton Pump Inhibitor examples include omeprazole (e.g. Losec, Prilosec), esomeprazole (e.g. Nexium), rabeprazole (e.g. Pariet, Aciphex), pantoprazole (e.g. Somac, Protonix) and lansoprazole (e.g. Zoton FasTabs, Prevacid). These drugs are not without their undesirable side effects. Side effects can include:
- Neutropenia (an unexplained decrease in the immune systems white cells that are involved in battling disease).[130]
- Pneumonia (infection of the lungs).[131]
- Vitamin B12 deficiency.[132],[133]
- Vitamin C and Iron deficiency.[134]
- Osteoporosis (a thinning and weakening of the bones leading to broken bones).[135],[136]
- Hip Fracture (broken hip).[137]
- Spine, forearm or wrist, and other fractures (broken bones).[138]
- Dementia (when the brain quits functioning and the memory is bad).[139]
- Depression (a downcast mood).[140]
- Chronic kidney disease (when the kidneys quit working).[141],[142]
- Hypomagnesaemia (low magnesium, a very important mineral for your body).[143]
- Hypoparathyroidism (low parathyroid function).[144]
- Tachycardia (fast heart rate).[145]
- Stomach infection with S. aureus, E. coli, Candida albicans (bad infections, hard to treat).[146]
- Slowed esophageal motility (when the esophagus has a hard time moving the food through to the stomach).[147]
The next most common drug prescribed for GERD is called an H2 antagonist. H2 antagonists are medications that block the action of histamine, (which usually increases inflammation), at its receptor site in the cells of the stomach. This decreases the production of stomach acid. H2 antagonist examples include famotidine (e.g.Pamacid, Pepzan, Pepcid), nizatidine (e.g. Tazac, Tacidine, Nizac, Axid), cimetidine (e.g. Magicul, Tagamet) and ranitidine (e.g. Zantac, Rani 2). These drugs are not without their undesirable side effects. Side effects can include:
- Neurotoxicity (damage to the nerve cells in your body or brain).[148]
- Overgrowth of Listeria monocytogenes (a dangerous bacteria).[149]
- Restless leg syndrome, and movement disorders (out of control muscle activity).[150]
- Bradycardia (very slow heart pumping rate).[151]
- Liver disease[152]
- Changes in the autonomic control of the heart (the heart goes out of control).[153]
A popular, over-the-counter GERD treatment is calcium carbonate. Calcium carbonate brand name examples include: Dicarbosil, Rolaids, Titralac, Tums. Calcium carbonate is not without its undesirable side effects. Side effects can include:
- "Acid rebound." (when, not long after you take the pill, the acid actually increases not decreases).[154]
- In some people it actually increases, not decreases, reflux.[155]
Natural Tips To Relieve GERD
If you are suffering with GERD you may find the following tips beneficial.
- · Maintain regularity in your meal schedule; eat at the exact same times every day.[156]
- · Eat small meals.
- · Take small bites and chew them well.
- · Eat lots of high fiber fresh fruits and vegetables.[157],[158]
- · Don’t drink any liquid with your meals.
- · Don’t make or eat liquid meals (soup, smoothies).
- · Drink 8-10 glasses of water a day: drink the water at least 30 minutes before meals or 2 hours after meals.
- · Leave at least five hours between your meals.
- · Eat only two meals a day (skip supper) and don’t snack. If you do eat supper eat only fresh fruit.
- · Take a short walk immediately after meals.[159]
- · Don’t eat with in 3-4 hours of going to bed.
- · Wear warm clothes that cover arms and legs well and have not tight bands around the waist.
- · Eat mainly low-fat, low-calorie foods.[160]
Natural Things To Help and Heal
If you are currently in pain and looking for things that could help relieve that pain or even contribute to healing, the following could be of assistance to you.
- · Charcoal capsules, tablets, or powder[161],[162]
- · Fruit, beans and vegetables[163]
- · Cabbage and its juice
- · Carrots
- · Broccoli, kale, radish, cucumber[164]
- · Broccoli sprouts
- · Pears
- · Bananas and kiwi[165]
- · Aloe Vera Juice
- · Carob
- · Dandelion tea
- · Fresh Comfrey[166]
Schedule Of The Day
So let’s take time and make this practical. What would a GERD sensitive lifestyle and diet look like? Now, I run the risk of having some sensitive soul with an allergy or food dislike getting bent out of shape over these recommendations, so this discussion will need to be seen as advisory and not compulsory or set in stone. What would a day possibly look like for someone trying to synthesize the forgoing information into a practical schedule? God made us to run on a schedule. Well, here goes:
5:00am Get out of bed. Drink one quart of warm water. Take a 15 minute walk outdoors.
6:30am Drink one cup of dandelion and/or comfrey tea.
7:00am Eat a breakfast of mostly fresh fruits (e.g. bananas, pears, kiwi, any fresh fruit)
Making a fruit salad and topping it with a nut cream is nice. (Nut cream recipe: In to a blender put 2/3 cup water, one tablespoon of one kind of seed [e.g. pumpkin seeds, sunflower seeds, flax seed, chia, hemp, sesame, etc], two tablespoons of one kind of nut [pecans, walnuts, almonds, brazil nuts, hazel nuts, etc. Avoid peanuts and cashews.], blend till creamy smooth and pour over the chopped fruit salad.)
Here is a really good oatmeal recipe for GERD: 2 cups water, ½ cup whole rolled oats [not quick or instant oats], ¼ cup oat bran, ¼ cup ground flax or chia, ¼ teaspoon salt. Bring water to a boil, add ingredients, simmer for a minimum of 45 minutes. Serve with your fruit salad and nut cream.
After Breakfast take a 15 minute walk outdoors.
10:00 am Drink another quart of water with one teaspoon of activated charcoal in it.
Take a short walk if possible.
12:30pm Drink another cup of dandelion and/or comfrey tea.
1:00pm Lunch: eat at the exact same time every day.
Keep in mind the forgoing dietary research for GERD. Concentrate on good vegetables, raw or steamed and less on prepared or complex foods. Avoid mixing fruits and vegetables at the same meal.
Chew your food well and don’t overeat.
See our website for some recipes: www.NorthernLightsHealthEducation.com
After lunch take a 15 minute walk outdoors.
3:30pm Drink one quart of water, no need to rush.
Take a short walk if possible.
6:00pm It would be best to skip supper,
but many can’t and with the proper precautions a good result can still be obtained. For supper eat only fresh fruit, chew it well and take a walk afterwards.
9:00pm Go to bed at 9:00pm
(even if you are not used to it, you can do it until it becomes a good habit.)
Changing the Tide
Not all diet and lifestyle changes are easy, especially when they go against favourite practices. I hope your favourite food is not on the list of causes of GERD. Habits can be changed and better health can be the result. For some, food, or their belly, can become more important to them than life itself. “For many walk, of whom I have told you often, and now tell you even weeping, that they are the enemies of the cross of Christ: Whose end is destruction, whose God is their belly, and whose glory is in their shame, who mind earthly things.”[167] On the other hand we are promised power to make positive changes. “I can do all things through Christ which strengtheneth me.” [168] So be true to yourself, stick with the program and reap the results.
[1] Yuan L, Tang D, Peng J, Qu N, Yue C, Wang F. Study on lifestyle in patients with gastroesophageal reflux disease. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2017 May 28;42(5):558-564.
[2] El-Serag HB, Sweet S, Winchester CC, and Dent J. Update on the epidemiology of gastro-oesophageal reflux disease: a systematic review. Gut. 2014 Jun; 63(6): 871–880.
[3] Lacy BE, Carter J, Weiss JE, Crowell MD. The effects of intraduodenal nutrient infusion on serum CCK, LES pressure, and gastroesophageal reflux. Neurogastroenterol Motil. 2011 Jul;23(7):631-e256.
[4] Babka JC, Castell DO. On the genesis of heartburn. The effects of specific foods on the lower esophageal sphincter. Am J Dig Dis. 1973 May;18(5):391-7.
[5] Kim YK1, Moon JS, Ryu SH, Lee JH, Kim YS. The relationship between the popular beverages in Korea and reported postprandial heartburn. Korean J Gastroenterol. 2010 Feb;55(2):109-18.
[6] Nagasaki A, Ishimori A, Masamune O, Yamagata S. Response of lower esophageal sphincter pressure to beef soup or AOC-tetrapeptide stimulation in esophagitis. Tohoku J Exp Med. 1977 Jan;121(1):91-7.
[7] Wright LE, Castell DO. The adverse effect of chocolate on lower esophageal sphincter pressure. Am J Dig Dis. 1975 Aug;20(8):703-7.
[8] Thomas FB, Steinbaugh JT, Fromkes JJ, Mekhjian HS, Caldwell JH. Inhibitory effect of coffee on lower esophageal sphincter pressure. Gastroenterology. 1980 Dec;79(6):1262-6.
[9] Gudjonsson H, McAuliffe TL, Kaye MD. The effect of coffee and tea upon lower esophageal sphincteric function. Laeknabladid. 1995 Jun;81(6):484-8.
[10] Braverman AS, Vegesna AK, Miller LS, Barbe MF, Tiwana M, Hussain K, Ruggieri MR Sr. Pharmacologic specificity of nicotinic receptor-mediated relaxation of muscarinic receptor precontracted human gastric clasp and sling muscle fibers within the gastroesophageal junction. J Pharmacol Exp Ther. 2011 Jul;338(1):37-46.
[11] Ness-Jensen E, Lagergren J. Tobacco smoking, alcohol consumption and gastro-oesophageal reflux disease. Best Pract Res Clin Gastroenterol. 2017 Oct;31(5):501-508.
[12] Kahrilas PJ. GERD pathogenesis, pathophysiology, and clinical manifestations. Cleve Clin J Med. 2003 Nov;70 Suppl 5:S4-19.
[13] Piche T, des Varannes SB, Sacher-Huvelin S, Holst JJ, Cuber JC, Galmiche JP. Colonic fermentation influences lower esophageal sphincter function in gastroesophageal reflux disease. Gastroenterology. 2003 Apr;124(4):894-902.
[14] Hamoui N, Lord RV, Hagen JA, Theisen J, Demeester TR, Crookes PF. Response of the lower esophageal sphincter to gastric distention by carbonated beverages. J Gastrointest Surg. 2006 Jun;10(6):870-7.
[15] Ford AC, Talley NJ, Walker MM, Jones MP. Increased prevalence of autoimmune diseases in functional gastrointestinal disorders: case-control study of 23471 primary care patients. Aliment Pharmacol Ther. 2014 Oct;40(7):827-34.
[16] Souza RF, Huo X, Mittal V, Schuler CM, Carmack SW, Zhang HY, Zhang X, Yu C, Hormi-Carver K, Genta RM, Spechler SJ. Gastroesophageal reflux might cause esophagitis through a cytokine-mediated mechanism rather than caustic acid injury. Gastroenterology. 2009 Nov;137(5):1776-84.
[17] Ferraz JG, Tigley AW, Appleyard CB, Wallace JL. TNF-alpha contributes to the pathogenesis of ethanol-induced gastric damage in cirrhotic rats. Am J Physiol. 1997 Apr;272(4 Pt 1):G809-14.
[18] Ramírez-Mayans JA, Toro-Monjaraz EM, Romero-Trujillo J, Cervantes-Bustamante R, Zárate-Mondragón F, Montijo-Barrios E, Cadena-León J, Cazares-Méndez M. 24-h intraesophageal pH determination in children allergic to cow's milk protein at a tertiary care hospital. Rev Gastroenterol Mex. 2014 Jan-Mar;79(1):3-6.
[19] Myers BM, Smith JL, Graham DY. Effect of red pepper and black pepper on the stomach. Am J Gastroenterol. 1987 Mar;82(3):211-4.
[20] Vasudevan K, Vembar S, Veeraraghavan K, Haranath PS. Influence of intragastric perfusion of aqueous spice extracts on acid secretion in anesthetized albino rats. Indian J Gastroenterol. 2000 Apr-Jun;19(2):53-6.
[21] v Schönfeld J, Evans DF. Fat, spices and gastro-oesophageal reflux. Z Gastroenterol. 2007 Feb;45(2):171-5.
[22] Kim YK, Moon JS, Ryu SH, Lee JH, Kim YS. The relationship between the popular beverages in Korea and reported postprandial heartburn. Korean J Gastroenterol. 2010 Feb;55(2):109-18.
[23] Feldman M, Barnett C. Relationships between the acidity and osmolality of popular beverages and reported postprandial heartburn. Gastroenterology. 1995 Jan;108(1):125-31.
[24] Drug induced lesions of the oesophageal mucosa. Prescrire Int. 2015 Sep;24(163):210-1, 213.
[25] Mungan Z, Pınarbaşı Şimşek B. Which drugs are risk factors for the development of gastroesophageal reflux disease? Turk J Gastroenterol. 2017 Dec;28(Suppl 1):S38-S43.
[26] Shibata T, Nakamura M, Omori T, Tahara T, Ichikawa Y, Okubo M, Ishizuka T, Nakagawa Y, Nagasaka M, Nakamura M, Arisawa T, Hirata I. Association between individual response to food taste and gastroesophageal symptoms. J Dig Dis. 2015 Jun;16(6):337-41.
[27] Riegler M, Kristo I, Asari R, Rieder E, Schoppmann SF. Dietary sugar and Barrett's esophagus. Eur Surg. 2017;49(6):279-281.
[28] Li N, Petrick JL, Steck SE, Bradshaw PT, McClain KM, Niehoff NM, Engel LS, Shaheen NJ, Corley DA, Vaughan TL, Gammon MD. Dietary sugar/starches intake and Barrett's esophagus: a pooled analysis. Eur J Epidemiol. 2017 Nov;32(11):1007-1017.
[29] Tasevska N, Jiao L, Cross AJ, Kipnis V, Subar AF, Hollenbeck A, Schatzkin A, Potischman N. Sugars in diet and risk of cancer in the NIH-AARP Diet and Health Study. Int J Cancer. 2012 Jan 1;130(1):159-69.
[30] Chirila I, Morariu ID, Barboi OB, Drug VL. The role of diet in the overlap between gastroesophageal reflux disease and functional dyspepsia. Turk J Gastroenterol. 2016 Jan;27(1):73-80.
[31] Fox M, Barr C, Nolan S, Lomer M, Anggiansah A, Wong T. The effects of dietary fat and calorie density on esophageal acid exposure and reflux symptoms. Clin Gastroenterol Hepatol. 2007 Apr;5(4):439-44.
[32] Saqui-Salces M, Dowdle WE, Reiter JF, Merchant JL. A high-fat diet regulates gastrin and acid secretion through primary cilia. FASEB J. 2012 Aug;26(8):3127-39.
[33] Alkhathami AM, Alzahrani AA, Alzhrani MA, Alsuwat OB, Mahfouz MEM. Risk Factors for Gastroesophageal Reflux Disease in Saudi Arabia. Gastroenterology Res. 2017 Oct;10(5):294-300.
[34] Arya V, Agarwal S, Singh S, Sison C, Gupta KA. The effect of increased chewing strokes on the DeMeester score. Dis Esophagus. 2017 May 1;30(5):1-5.
[35] Sarosiek J, Scheurich CJ, Marcinkiewicz M, McCallum RW. Enhancement of salivary esophagoprotection: rationale for a physiological approach to gastroesophageal reflux disease. Gastroenterology. 1996 Mar;110(3):675-81.
[36] Takeshita E, Furukawa S, Sakai T, Niiya T, Miyaoka H, Miyake T, Yamamoto S, Senba H, Yamamoto Y, Arimitsu E, Yagi S, Utsunomiya H, Tanaka K, Ikeda Y, Matsuura B, Miyake Y, Hiasa Y. Eating Behaviours and Prevalence of Gastroesophageal Reflux Disease in Japanese Patients with Type 2 Diabetes Mellitus: The Dogo Study. Can J Diabetes. 2017 Oct 19. pii: S1499-2671(17)30130-2.
[37] Nathanson BH, Navab F. An Analysis of Weight Gains and Body Mass Index in Patients with Barrett's Esophagus. J Acad Nutr Diet. 2016 Jul;116(7):1156-62.
[38] Gudjonsson H, McAuliffe TL, Kaye MD. The effect of coffee and tea upon lower esophageal sphincteric function. Laeknabladid. 1995 Jun;81(6):484-8.
[39] Kaufman SE, Kaye MD. Induction of gastro-oesophageal reflux by alcohol. Gut. 1978 Apr;19(4):336-8.
[40] Walsh NP, Laing SJ, Oliver SJ, Montague JC, Walters R, Bilzon JL. Saliva parameters as potential indices of hydration status during acute dehydration. Med Sci Sports Exerc. 2004 Sep;36(9):1535-42.
[41] Decktor DL, Robinson M, Maton PN, Lanza FL, Gottlieb S. Effects of Aluminum/Magnesium Hydroxide and Calcium Carbonate on Esophageal and Gastric pH in Subjects with Heartburn. Am J Ther. 1995 Aug;2(8):546-552.
[42] Fischbach LA, Correa P, Feldman M, Fontham E, Priest E, Goodman KJ, Jain R. Increased reflux symptoms after calcium carbonate supplementation and successful anti-Helicobacter pylori treatment. Dig Dis Sci. 2003 Aug;48(8):1487-94.
[43] Campanozzi A, Capano G, Miele E, Romano A, Scuccimarra G, Del Giudice E, Strisciuglio C, Militerni R, Staiano A. Impact of malnutrition on gastrointestinal disorders and gross motor abilities in children with cerebral palsy. Brain Dev. 2007 Jan;29(1):25-9.
[44] Weijenborg PW, Smout AJ, Verseijden C, van Veen HA, Verheij J, de Jonge WJ, Bredenoord AJ. Hypersensitivity to acid is associated with impaired esophageal mucosal integrity in patients with gastroesophageal reflux disease with and without esophagitis. Am J Physiol Gastrointest Liver Physiol. 2014 Aug 1;307(3):G323-9.
[45] Grønbech JE, Lacy ER. Role of gastric blood flow in impaired defense and repair of aged rat stomachs. Am J Physiol. 1995 Nov;269(5 Pt 1):G737-44.
[46] Grönbech JE, Matre K, Stangeland L, Svanes K, Varhaug JE. Gastric mucosal repair in the cat: role of the hyperemic response to mucosal damage. Gastroenterology. 1988 Aug;95(2):311-20.
[47] Ayazi S, Tamhankar A, DeMeester SR, Zehetner J, Wu C, Lipham JC, Hagen JA, DeMeester TR. The impact of gastric distension on the lower esophageal sphincter and its exposure to acid gastric juice. Ann Surg. 2010 Jul;252(1):57-62.
[48] Lara FJ, Carranque G, Oehling H, Hernández JM, Oliva H. Psychological modulation in patients surgically intervened for gastroesophageal reflux disease. Dis Esophagus. 2014 Aug;27(6):538-46.
[49] Holtmann G, Kriebel R, Singer MV. Mental stress and gastric acid secretion. Do personality traits influence the response? Dig Dis Sci. 1990 Aug;35(8):998-1007.
[50] Wu KL, Rayner CK, Chuah SK, Chiu YC, Chiu KW, Hu TH, Chiu CT. Effect of liquid meals with different volumes on gastroesophageal reflux disease. J Gastroenterol Hepatol. 2014 Mar;29(3):469-73.
[51] Proverbs 23:2, King James Version of the Holy Bible.
[52] Randhawa MA, Yar T, Gillessen A. An effective and physiological lifestyle change for management of gastroesophageal reflux disease. J Ayub Med Coll Abbottabad. 2013 Jan-Jun;25(1-2):206-7.
[53] Jackson SJ, Leahy FE, Jebb SA, Prentice AM, Coward WA, Bluck LJ. Frequent feeding delays the gastric emptying of a subsequent meal. Appetite. 2007 Mar;48(2):199-205. Epub 2006 Nov 1.
[54] Reshetnikov OV, Kurilovich SA, Denisov MIu. Mode of dieting as a risk factor for dyspeptic symptoms: a two-year prospective study. Vopr Pitan. 2010;79(2):39-42.
[55] Pera P, Bucca C, Borro P, Bernocco C, De LA, Carossa S. Influence of mastication on gastric emptying. J Dent Res. 2002 Mar;81(3):179-81.
[56] Horowitz M, Maddox A, Bochner M, Wishart J, Bratasiuk R, Collins P, Shearman D. Relationships between gastric emptying of solid and caloric liquid meals and alcohol absorption. Am J Physiol. 1989 Aug;257(2 Pt 1):G291-8.
[57] Edelbroek M, Horowitz M, Maddox A, Bellen J. Gastric emptying and intragastric distribution of oil in the presence of a liquid or a solid meal. J Nucl Med. 1992 Jul;33(7):1283-90.
[58] Meyer JH, Elashoff JD, Lake R. Gastric emptying of indigestible versus digestible oils and solid fats in normal humans. Dig Dis Sci. 1999 Jun;44(6):1076-82.
[59] Benini L, Brighenti F, Castellani G, Brentegani MT, Casiraghi MC, Ruzzenente O, Sembenini C, Pellegrini N, Caliari S, Porrini M, et al. Gastric emptying of solids is markedly delayed when meals are fried. Dig Dis Sci. 1994 Nov;39(11):2288-94.
[60] Peracchi M, Gebbia C, Ogliari C, Fraquelli M, Viganò R, Baldassarri A, Bianchi PA, Conte D. Influence of caloric intake on gastric emptying of solids assessed by 13C-octanoic acid breath test. Scand J Gastroenterol. 2000 Aug;35(8):814-8.
[61] Troncon LE, Iazigi N. Effect of test meal temperature on the gastric emptying of liquids. Braz J Med Biol Res. 1988;21(1):57-60.
[62] Scott AM, Kellow JE, Eckersley GM, Nolan JM, Jones MP. Cigarette smoking and nicotine delay postprandial mouth-cecum transit time. Dig Dis Sci. 1992 Oct;37(10):1544-7.
[63] Franke A, Nakchbandi IA, Schneider A, Harder H, Singer MV. The effect of ethanol and alcoholic beverages on gastric emptying of solid meals in humans. Alcohol Alcohol. 2005 May-Jun;40(3):187-93.
[64] Horowitz M, Maddox A, Bochner M, Wishart J, Bratasiuk R, Collins P, Shearman D. Relationships between gastric emptying of solid and caloric liquid meals and alcohol absorption. Am J Physiol. 1989 Aug;257(2 Pt 1):G291-8.
[65] Podczeck F, Mitchell CL, Newton JM, Evans D, Short MB. The gastric emptying of food as measured by gamma-scintigraphy and electrical impedance tomography (EIT) and its influence on the gastric emptying of tablets of different dimensions. J Pharm Pharmacol. 2007 Nov;59(11):1527-36.
[66] Jackson SJ, Leahy FE, Jebb SA, Prentice AM, Coward WA, Bluck LJ. Frequent feeding delays the gastric emptying of a subsequent meal. Appetite. 2007 Mar;48(2):199-205. Epub 2006 Nov 1.
[67] Moore JG; Datz FL; Christian PE; Greenberg E; Alazraki N. Effect of body posture on radionuclide measurements of gastric emptying. Dig Dis Sci. 1988; 33(12):1592-5.
[68] Goo RH, Moore JG, Greenberg E, Alazraki NP. Circadian variation in gastric emptying of meals in humans. Gastroenterology. 1987 Sep;93(3):515-8.
[69] Kalkan Ç, Soykan I, Soydal Ç, Özkan E, Kalkan E. Assessment of Gastric Emptying in Patients with Autoimmune Gastritis. Dig Dis Sci. 2016 Jun;61(6):1597-602.
[70] Murray R. The effects of consuming carbohydrate-electrolyte beverages on gastric emptying and fluid absorption during and following exercise. Sports Med. 1987 Sep-Oct;4(5):322-51.
[71] Roland J, Dobbeleir A, Vandevivere J, Ham HR. Effect of mild mental stress on solid phase gastric emptying in healthy subjects. Nucl Med Commun. 1990 Apr;11(4):319-26.
[72] Okholm M, Jensen SM. Gatroesophageal reflux in pregnant women. Ugeskr Laeger. 1995 Mar 27;157(13):1835-8.
[73] Salovaara S, Larsson Alminger M, Eklund-Jonsson C, Andlid T, Sandberg AS. Prolonged transit time through the stomach and small intestine improves iron dialyzability and uptake in vitro. J Agric Food Chem. 2003 Aug 13;51(17):5131-6.
[74] Kelsay JL; Behall KM; Prather ES Effect of fiber from fruits and vegetables on metabolic responses of human subjects I. Bowel transit time, number of defecations, fecal weight, urinary excretions of energy and nitrogen and apparent digestibilities of energy, nitrogen, and fat. Am J Clin Nutr 1978 Jul;31(7):1149-53.
[75] Erbil Y, Berber E, Seven R, et. al. The effect of intestinal transit time on bacterial translocation. Acta Chir Belg. 1998 Dec;98(6):245-9.
[76] Wigg AJ; Roberts-Thomson IC; Dymock RB, et. al. The role of small intestinal bacterial overgrowth, intestinal permeability, endotoxaemia, and tumour necrosis factor alpha in the pathogenesis of non-alcoholic steatohepatitis. Gut 2001 Feb;48(2):206-11.
[77] Bauer TM; Schwacha H; Steinbruckner B; et. al. Small intestinal bacterial overgrowth in human cirrhosis is associated with systemic endotoxemia. Am J Gastroenterol 2002 Sep;97(9):2364-70.
[78]Spaeth G, Berg RD, Specian RD, et. al. Food without fiber promotes bacterial translocation from the gut. Surgery. 1990 Aug;108(2):240-6; discussion 246-7.
[79] Roen PB. The evening meal and atherosclerosis. J Am Geriatr Soc 1978 Jun;26(6):284-5.
[80] Gogler H. Intestinal transit time in Togo (Western Africa) and Germany. Z Gastroenterol. 1976 Apr;14(2):280-4.
[81] Spiller GA, Story JA, Wong LG, et.al. Effect of increasing levels of hard wheat fiber on fecal weight, minerals and
steroids and gastrointestinal transit time in healthy young women. J Nutr. 1986 May;116(5):778-85.
[82] Spiller GA, Story JA, Lodics TA, et. al. Effect of sun-dried raisins on bile acid excretion, intestinal transit time, and
fecal weight: a dose-response study. J Med Food. 2003 Summer;6(2):87-91.
[83] Anitha M, Reichardt F, Tabatabavakili S, Nezami BG, Chassaing B, Mwangi S, Vijay-Kumar M, Gewirtz A, Srinivasan S. Intestinal dysbiosis contributes to the delayed gastrointestinal transit in high-fat diet fed mice. Cell Mol Gastroenterol Hepatol. 2016 May;2(3):328-339.
[84] Kelsay JL, Behall KM, Prather ES. Effect of fiber from fruits and vegetables on metabolic responses of human subjects I. Bowel transit time, number of defecations, fecal weight, urinary excretions of energy and nitrogen and apparent digestibilities of energy, nitrogen, and fat. Am J Clin Nutr. 1978 Jul;31(7):1149-53.
[85] Chaudhary HR. Study of intestinal transit time in patient with anxiety and depression. J Assoc Physicians India. 1989 Feb;37(2):156-7.
[86] Yuan L, Tang D, Peng J, Qu N, Yue C, Wang F. Study on lifestyle in patients with gastroesophageal reflux disease. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2017 May 28;42(5):558-564.
[87] Stanich PP, Peck J, Murphy C, Porter KM, Meyer MM. Physical activity during video capsule endoscopy correlates with shorter bowel transit time. Endosc Int Open. 2017 Sep;5(9):E856-E860.
[88] Kim JH. The physical activity level in female affects colon transit time. J Neurogastroenterol Motil. 2012 Jan;18(1):4-5.
[89] Morley JE, Levine AS, Yamada T, Gebhard RL, Prigge WF, Shafer RB, Goetz FC, Silvis SE. Effect of exorphins on gastrointestinal function, hormonal release, and appetite. Gastroenterology. 1983 Jun;84(6):1517-23.
[90] Chiarioni G, Bassotti G, Germani U, Battaglia E, Brentegani MT, Morelli A, Vantini I. Gluten-free diet normalizes mouth-to-cecum transit of a caloric meal in adult patients with celiac disease. Dig Dis Sci. 1997 Oct;42(10):2100-5.
[91] Haug A, Høstmark AT, Harstad OM. Bovine milk in human nutrition--a review. Lipids Health Dis. 2007 Sep 25;6:25.
[92] Zheng Y, Hu J, Murphy PA, Alekel DL, Franke WD, Hendrich S. Rapid gut transit time and slow fecal isoflavone disappearance phenotype are associated with greater genistein bioavailability in women. J Nutr. 2003 Oct;133(10):3110-6.
[93] Gögler H. Intestinal transit time in Togo (Western Africa) and Germany. Z Gastroenterol. 1976 Apr;14(2):280-4.
[94] Bhate PA, Patel JA, Parikh P, Ingle MA, Phadke A, Sawant PD. Total and Segmental Colon Transit Time Study in Functional Constipation: Comparison With Healthy Subjects. Gastroenterology Res. 2015 Feb;8(1):157-159.
[95] Jahng J, Jung IS, Choi EJ, Conklin JL, Park H. The effects of methane and hydrogen gases produced by enteric bacteria on ileal motility and colonic transit time. Neurogastroenterol Motil. 2012 Feb;24(2):185-90, e92.
[96] Neurogastroenterol Motil. 2007 Feb;19(2):94-102. Impedance monitoring shows that posture and a meal influence gastro-oesophageal reflux composition and frequency. Shay SS, Lopez R.
[97]Caselli M, Zuliani G, Cassol F, Fusetti N, Zeni E, Lo Cascio N, Soavi C, Gullini S. Test-based exclusion diets in gastro-esophageal reflux disease patients: a randomized controlled pilot trial. World J Gastroenterol. 2014 Dec 7;20(45):17190-5.
[98] Niu CY, Zhou YL, Yan R, Mu NL, Gao BH, Wu FX, Luo JY. Incidence of gastroesophageal reflux disease in Uygur and Han Chinese adults in Urumqi. World J Gastroenterol. 2012 Dec 28;18(48):7333-40.
[99] Huang W, Han Y, Xu J, Zhu W, Li Z. Red and processed meat intake and risk of esophageal adenocarcinoma: a meta-analysis of observational studies. Cancer Causes Control. 2013 Jan;24(1):193-201.
[100] Chung CH. Corrosive oesophageal injury following vinegar ingestion. Hong Kong Med J. 2002 Oct;8(5):365-6.
[101] Dryahina K, Pospíšilová V, Sovová K, Shestivska V, Kubišta J, Spesyvyi A, Pehal F, Turzíková J, Votruba J, Spaněl P. Exhaled breath concentrations of acetic acid vapour in gastro-esophageal reflux disease. J Breath Res. 2014 Sep;8(3):037109.
[102] Surdea-Blaga T, Negrutiu DE, Palage M, Dumitrascu DL. Food and Gastroesophageal Reflux Disease. Curr Med Chem. 2017 May 15.
[103] Dai Q, Cantwell MM, Murray LJ, Zheng W, Anderson LA, Coleman HG; FINBAR study group. Dietary magnesium, calcium:magnesium ratio and risk of reflux oesophagitis, Barrett's oesophagus and oesophageal adenocarcinoma: a population-based case-control study. Br J Nutr. 2016 Jan 28;115(2):342-50.
[104] Murphy SJ, Anderson LA, Ferguson HR, Johnston BT, Watson PR, McGuigan J, Comber H, Reynolds JV, Murray LJ, Cantwell MM. Dietary antioxidant and mineral intake in humans is associated with reduced risk of esophageal adenocarcinoma but not reflux esophagitis or Barrett's esophagus. J Nutr. 2010 Oct;140(10):1757-63.
[105] Mercer CD, Rue C, Hanelin L, Hill LD. Effect of obesity on esophageal transit. Am J Surg. 1985 Jan;149(1):177-81.
[106] Drug induced lesions of the oesophageal mucosa. Prescrire Int. 2015 Sep;24(163):210-1, 213.
[107] Wright CE, Ebrecht M, Mitchell R, Anggiansah A, Weinman J. The effect of psychological stress on symptom severity and perception in patients with gastro-oesophageal reflux. J Psychosom Res. 2005 Dec;59(6):415-24.
[108] Eherer A. Management of gastroesophageal reflux disease: lifestyle modification and alternative approaches. Dig Dis. 2014;32(1-2):149-51.
[109] Ito Y, Suzuki K, Ichino N, Imai H, Sakaguchi H, Hokama M, Nishii M, Nakano H. The Risk of Helicobacter Pylori Infection and Atrophic Gastritis from Food and Drink Intake: a Cross-sectional Study in Hokkaido, Japan. Asian Pac J Cancer Prev. 2000;1(2):147-156.
[110] Riegler M, Kristo I, Asari R, Rieder E, Schoppmann SF. Dietary sugar and Barrett's esophagus. Eur Surg. 2017;49(6):279-281.
[111] Li N, Petrick JL, Steck SE, Bradshaw PT, McClain KM, Niehoff NM, Engel LS, Shaheen NJ, Corley DA, Vaughan TL, Gammon MD. Dietary sugar/starches intake and Barrett's esophagus: a pooled analysis. Eur J Epidemiol. 2017 Nov;32(11):1007-1017.
[112] Schneider JL, Corley DA. The Troublesome Epidemiology of Barrett's Esophagus and Esophageal Adenocarcinoma. Gastrointest Endosc Clin N Am. 2017 Jul;27(3):353-364.
[113] Shivappa N, Hebert JR, Anderson LA, Shrubsole MJ, Murray LJ, Getty LB, Coleman HG. Dietary inflammatory index and risk of reflux oesophagitis, Barrett's oesophagus and oesophageal adenocarcinoma: a population-based case-control study. Br J Nutr. 2017 May;117(9):1323-1331.
[114] Nathanson BH, Navab F. An Analysis of Weight Gains and Body Mass Index in Patients with Barrett's Esophagus. J Acad Nutr Diet. 2016 Jul;116(7):1156-62.
[115] Sun L, Zhang Z, Xu J, Xu G, Liu X. Dietary fiber intake reduces risk for Barrett's esophagus and esophageal cancer. Crit Rev Food Sci Nutr. 2017 Sep 2;57(13):2749-2757.
[116] Petrick JL, Steck SE, Bradshaw PT, Chow WH, Engel LS, He K, Risch HA, Vaughan TL, Gammon MD. Dietary flavonoid intake and Barrett's esophagus in western Washington State. Ann Epidemiol. 2015 Oct;25(10):730-5.e2.
[117] Lee YY, McColl KE. Disruption of the gastroesophageal junction by central obesity and waist belt: role of raised intra-abdominal pressure. Dis Esophagus. 2015 May-Jun;28(4):318-25.
[118] Jiao L, Kramer JR, Chen L, Rugge M, Parente P, Verstovsek G, Alsarraj A, El-Serag HB. Dietary consumption of meat, fat, animal products and advanced glycation end-products and the risk of Barrett's oesophagus. Aliment Pharmacol Ther. 2013 Oct;38(7):817-24.
[119] Jiao L, Kramer JR, Rugge M, Parente P, Verstovsek G, Alsarraj A, El-Serag HB. Dietary intake of vegetables, folate, and antioxidants and the risk of Barrett's esophagus. Cancer Causes Control. 2013 May;24(5):1005-14.
[120] Ibiebele TI, Hughes MC, Nagle CM, Bain CJ, Whiteman DC, Webb PM; Study of Digestive Health and Australian Cancer Study. Dietary antioxidants and risk of Barrett's esophagus and adenocarcinoma of the esophagus in an Australian population. Int J Cancer. 2013 Jul;133(1):214-24.
[121] Murphy SJ, Anderson LA, Ferguson HR, Johnston BT, Watson PR, McGuigan J, Comber H, Reynolds JV, Murray LJ, Cantwell MM. Dietary antioxidant and mineral intake in humans is associated with reduced risk of esophageal adenocarcinoma but not reflux esophagitis or Barrett's esophagus. J Nutr. 2010 Oct;140(10):1757-63.
[122] Kubo A, Corley DA, Jensen CD, Kaur R. Dietary factors and the risks of oesophageal adenocarcinoma and Barrett's oesophagus. Nutr Res Rev. 2010 Dec;23(2):230-46.
[123] Chen KH, Mukaisho K, Sugihara H, Araki Y, Yamamoto G, Hattori T. High animal-fat intake changes the bile-acid composition of bile juice and enhances the development of Barrett's esophagus and esophageal adenocarcinoma in a rat duodenal-contents reflux model. Cancer Sci. 2007 Nov;98(11):1683-8.
[124] Anderson LA, Watson RG, Murphy SJ, Johnston BT, Comber H, Mc Guigan J, Reynolds JV, Murray LJ. Risk factors for Barrett's oesophagus and oesophageal adenocarcinoma: results from the FINBAR study. World J Gastroenterol. 2007 Mar 14;13(10):1585-94.
[125] Moe GL, Kristal AR, Levine DS, Vaughan TL, Reid BJ. Waist-to-hip ratio, weight gain, and dietary and serum selenium are associated with DNA content flow cytometry in Barrett's esophagus. Nutr Cancer. 2000;36(1):7-13.
[126] Van Cutsem E, Vantrappen G. Epidemiology and clinical aspects of esophageal cancer. J Belge Radiol. 1991;74(5):365-8.
[127] Huang W, Han Y, Xu J, Zhu W, Li Z. Red and processed meat intake and risk of esophageal adenocarcinoma: a meta-analysis of observational studies. Cancer Causes Control. 2013 Jan;24(1):193-201.
[128] Miller G, Wong C, Pollack A. Gastro-oesophageal reflux disease (GORD) in Australian general practice patients. Aust Fam Physician. 2015 Oct;44(10):701-4.
[129] Hollingworth S, Duncan EL, Martin JH. Marked increase in proton pump inhibitors use in Australia. Pharmacoepidemiol Drug Saf. 2010 Oct;19(10):1019-24.
[130] Gouraud A, Vochelle V, Descotes J, Vial T. Proton pump inhibitor-induced neutropenia: possible cross-reactivity between omeprazole and pantoprazole. Clin Drug Investig. 2010;30(8):559-63.
[131] Canani RB, Cirillo P, Roggero P, Romano C, Malamisura B, Terrin G, Passariello A, Manguso F, Morelli L, Guarino A; Working Group on Intestinal Infections of the Italian Society of Pediatric Gastroenterology, Hepatology and Nutrition (SIGENP). Therapy with gastric acidity inhibitors increases the risk of acute gastroenteritis and community-acquired pneumonia in children. Pediatrics. 2006 May;117(5):e817-20.
[132] Valuck RJ, Ruscin JM. A case-control study on adverse effects: H2 blocker or proton pump inhibitor use and risk of vitamin B12 deficiency in older adults. J Clin Epidemiol. 2004 Apr;57(4):422-8.
[133] Ruscin JM, Page RL 2nd, Valuck RJ. Vitamin B(12) deficiency associated with histamine(2)-receptor antagonists and a proton-pump inhibitor. Ann Pharmacother. 2002 May;36(5):812-6.
[134] McColl KE. Effect of proton pump inhibitors on vitamins and iron. Am J Gastroenterol. 2009 Mar;104 Suppl 2:S5-9.
[135] Lin SM, Yang SH, Liang CC, Huang HK. Proton pump inhibitor use and the risk of osteoporosis and fracture in stroke patients: a population-based cohort study. Osteoporos Int. 2018 Jan;29(1):153-162.
[136] Jacob L, Hadji P, Kostev K. The use of proton pump inhibitors is positively associated with osteoporosis in postmenopausal women in Germany. Climacteric. 2016 Oct;19(5):478-81.
[137] Yang YX, Lewis JD, Epstein S, Metz DC. Long-term proton pump inhibitor therapy and risk of hip fracture. JAMA. 2006 Dec 27;296(24):2947-53.
[138] Gray SL, LaCroix AZ, Larson J, Robbins J, Cauley JA, Manson JE, Chen Z. Proton pump inhibitor use, hip fracture, and change in bone mineral density in postmenopausal women: results from the Women's Health Initiative. Arch Intern Med. 2010 May 10;170(9):765-71.
[139] Gomm W, von Holt K, Thomé F, Broich K, Maier W, Fink A, Doblhammer G, Haenisch B. Association of Proton Pump Inhibitors With Risk of Dementia: A Pharmacoepidemiological Claims Data Analysis. JAMA Neurol. 2016 Apr;73(4):410-6.
[140] Laudisio A, Antonelli Incalzi R, Gemma A, Giovannini S, Lo Monaco MR, Vetrano DL, Padua L, Bernabei R, Zuccalà G. Use of proton-pump inhibitors is associated with depression: a population-based study. Int Psychogeriatr. 2018 Jan;30(1):153-159.
[141] Lazarus B, Chen Y, Wilson FP, Sang Y, Chang AR, Coresh J, Grams ME. Proton Pump Inhibitor Use and the Risk of Chronic Kidney Disease. JAMA Intern Med. 2016 Feb;176(2):238-46.
[142] Klatte DCF, Gasparini A, Xu H, de Deco P, Trevisan M, Johansson ALV, Wettermark B, Ärnlöv J, Janmaat CJ, Lindholm B, Dekker FW, Coresh J, Grams ME, Carrero JJ. Association Between Proton Pump Inhibitor Use and Risk of Progression of Chronic Kidney Disease. Gastroenterology. 2017 Sep;153(3):702-710.
[143] Cundy T, Dissanayake A. Severe hypomagnesaemia in long-term users of proton-pump inhibitors. Clin Endocrinol (Oxf). 2008 Aug;69(2):338-41.
[144] Swaminathan K. Proton pump inhibitor-induced hypomagnesemic hypoparathyroidism. Indian J Pharmacol. 2015 May-Jun;47(3):330-1.
[145] Elliott EM. The Relationship Between Resistant Tachycardia and Treatment for GERD. Explore (NY). 2016 Nov - Dec;12(6):456-458.
[146] Gościmski A, Matras J, Wallner G. Microflora of gastric juice in patients after eradication of Helicobacter pylori and treatment with a proton pump inhibitor. Wiad Lek. 2002;55(1-2):19-28.
[147] Fouad YM, Katz PO, Castell DO. Oesophageal motility defects associated with nocturnal gastro-oesophageal reflux on proton pump inhibitors. Aliment Pharmacol Ther. 1999 Nov;13(11):1467-71.
[148] Kawakami J, Yamamoto K, Shimokawa M, Sawada Y, Asanuma A, Yanagisawa K, Iga T. Neurotoxic study of H2 antagonists using Xenopus oocytes injected with mouse-brain mRNA. Biol Pharm Bull. 1997 Sep;20(9):1030-2.
[149] Cobb CA, Curtis GD, Bansi DS, Slade E, Mehal W, Mitchell RG, Chapman RW. Increased prevalence of Listeria monocytogenes in the faeces of patients receiving long-term H2-antagonists. Eur J Gastroenterol Hepatol. 1996 Nov;8(11):1071-4.
[150] O'Sullivan RL, Greenberg DB. H2 antagonists, restless leg syndrome, and movement disorders. Psychosomatics. 1993 Nov-Dec;34(6):530-2.
[151] Tanner LA, Arrowsmith JB. Bradycardia and H2 antagonists. Ann Intern Med. 1988 Sep 1;109(5):434-5.
[152] Bassan H, Zimmerman HJ, Jacob L, Gillespie J, Lukacs L. Effects of three H2 antagonists on the isolated perfused rat liver. Correlation of bile flow changes with potential for causing hepatic disease in patients. Biochem Pharmacol. 1986 Dec 15;35(24):4519-22.
[153] Nault MA, Milne B, Parlow JL. Effects of the selective H1 and H2 histamine receptor antagonists loratadine and ranitidine on autonomic control of the heart. Anesthesiology. 2002 Feb;96(2):336-41.
[154] Decktor DL, Robinson M, Maton PN, Lanza FL, Gottlieb S. Effects of Aluminum/Magnesium Hydroxide and Calcium Carbonate on Esophageal and Gastric pH in Subjects with Heartburn. Am J Ther. 1995 Aug;2(8):546-552.
[155] Fischbach LA, Correa P, Feldman M, Fontham E, Priest E, Goodman KJ, Jain R. Increased reflux symptoms after calcium carbonate supplementation and successful anti-Helicobacter pylori treatment. Dig Dis Sci. 2003 Aug;48(8):1487-94.
[156] Esmaillzadeh A, Keshteli AH, Feizi A, Zaribaf F, Feinle-Bisset C, Adibi P. Patterns of diet-related practices and prevalence of gastro-esophageal reflux disease. Neurogastroenterol Motil. 2013 Oct;25(10):831-e638.
[157] Keshteli AH, Shaabani P, Tabibian SR, Saneei P, Esmaillzadeh A, Adibi P. The relationship between fruit and vegetable intake with gastroesophageal reflux disease in Iranian adults. J Res Med Sci. 2017 Nov 28;22:125.
[158] Kubo A, Levin TR, Block G, Rumore GJ, Quesenberry CP Jr, Buffler P, Corley DA. Dietary antioxidants, fruits, and vegetables and the risk of Barrett's esophagus. Am J Gastroenterol. 2008 Jul;103(7):1614-23.
[159] Avidan B, Sonnenberg A, Schnell TG, Sontag SJ. Walking and chewing reduce postprandial acid reflux. Aliment Pharmacol Ther. 2001 Feb;15(2):151-5.
[160] Parker HL, Curcic J, Heinrich H, Sauter M, Hollenstein M, Schwizer W, Savarino E, Fox M. What to eat and drink in the festive season: a pan-European, observational, cross-sectional study. Eur J Gastroenterol Hepatol. 2017 May;29(5):608-614.
[161] Coffin B, Bortolloti C, Bourgeois O, Denicourt L. Efficacy of a simethicone, activated charcoal and magnesium oxide combination (Carbosymag®) in functional dyspepsia: results of a general practice-based randomized trial. Clin Res Hepatol Gastroenterol. 2011 Jun;35(6-7):494-9.
[162] https://www.buyactivatedcharcoal.com
[163] Nam SY, Park BJ, Cho YA, Ryu KH, Choi IJ, Park S, Kim YW. Different effects of dietary factors on reflux esophagitis and non-erosive reflux disease in 11,690 Korean subjects. J Gastroenterol. 2017 Jul;52(7):818-829.
[164] Panda V, Shinde P, Deora J, Gupta P. A comparative study of the antacid effect of some commonly consumed foods for hyperacidity in an artificial stomach model. Complement Ther Med. 2017 Oct;34:111-115.
[165] Hajizadeh B, Jessri M, Moasheri SM, Rad AH, Rashidkhani B. Fruits and vegetables consumption and esophageal squamous cell carcinoma: a case-control study. Nutr Cancer. 2011;63(5):707-13.
[166] Shipard, Isabell. How Can I Use Herbs in My Daily Life? Australia, David Stewart: 2013.
[167] Philippians 3:18-19, King James Version of the Holy Bible.
[168] Ibid 4:13.